There have been profoundly serious concerns in recent times on the safety of vaginal sling surgery for the management of stress urinary incontinence. The brouhaha around the use of the mesh reached its zenith with the banning of the use of mesh for SUI surgery in the UK. There are indications that sling surgery for SUI may be reintroduced in the UK, albeit with regulation and caveats in place. Given the controversy, there is no doubt that it is imperative that we understand sling behavior in vivo and factors underlying sling success. Transperineal and endovaginal 2D and 3D multicompartment ultrasound imaging of slings is evolving into a useful tool in the assessment of post-implantation sling behavior including determining etiology of failure following surgery (Hegde et al 2020). This article looks at two factors that potentially impact success of sling surgery: location of sling and dynamic in vivo behavior.
Figures 1, 2, and 3 are mid sagittal plane cut sections of 3D cubes obtained of the anterior pelvic compartment using an endovaginal transducer (BK Profocus Ultraview, Peabody, MA).
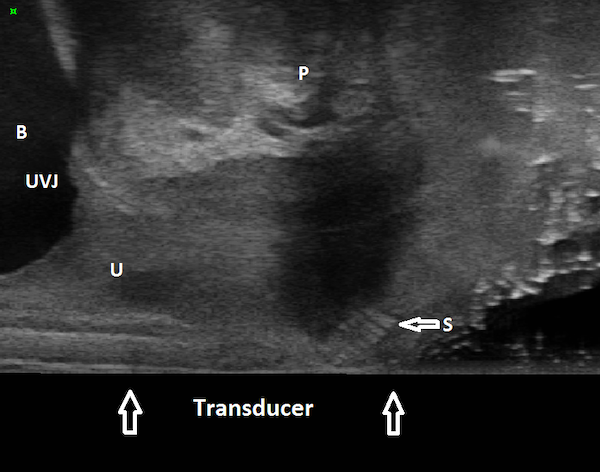
Figure 1
Endovaginal 180 degrees anterior compartment image in the midsagittal plane (transducer in the vagina scanning anteriorly): transobturator sling is seen to lie mid-urethrally. B: Bladder; U: Urethra; S: Sling; UVJ: Urethrovesical junction; P: Symphysis pubis
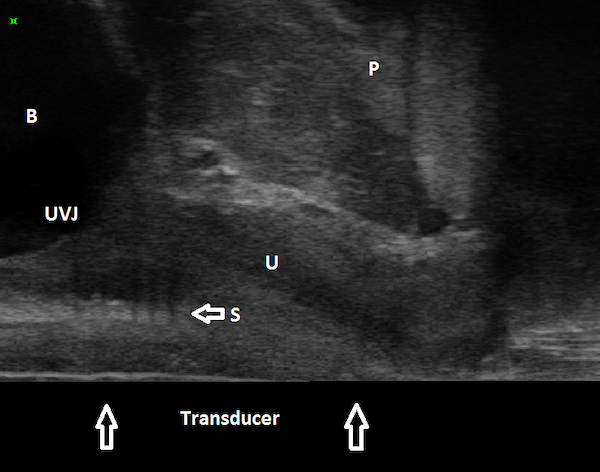
Figure 2
Endovaginal 180 degrees anterior compartment image in the midsagittal plane (transducer in the vagina scanning anteriorly): transobturator sling is seen to lie beneath proximal urethra B: Bladder; U: Urethra; S: Sling; UVJ: Urethrovesical junction; P: Symphysis pubis
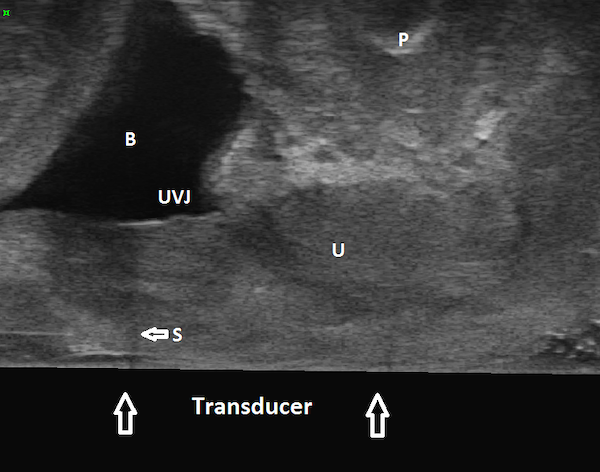
Figure 3
Endovaginal 180 degrees anterior compartment image in the midsagittal plane (transducer in the vagina scanning anteriorly): transobturator sling is seen to lie proximal to urethrovesical junction. B: Bladder; U: Urethra; S: Sling; UVJ: Urethrovesical junction; P: Symphysis pubis
The sling can be seen located mid-urethrally in Figure 1, underneath proximal urethra in Figure 2, and proximal to the urethrovesical junction in Figure 3, a year after surgery. Whether sling location impacts surgical outcome is a matter of controversy. Dietz et al (2004) concluded that variations in sling placement have little effect on symptom resolution and patient satisfaction in a study of 142 women whose outcomes were evaluated 5 weeks to 2.1 years following TVT sling surgery. Using transperineal ultrasound, the tape position in their study was found to vary from 30 mm above to 12.7 mm below the symphysis pubis at rest and between 15 mm above to 18.7 mm below the symphysis pubis on Valsalva. However, in an unmatched case-control study of 100 patients who underwent Monarc transobturator sling surgery, our group found that the sling location was significantly more proximal in those who had failed sling surgery when compared with those who had succeeded. In 90% of the patients in whom the sling had favorable outcomes, the sling was found to be located either beneath the ‘high pressure zone’ of mid-urethra or at the junction of the proximal and mid urethra (Hegde et al 2013).
The key differentiator in two studies is the fact that Dietz et al (2004) have used the symphysis pubis as the reference point for determining sling location; they measured the distance of the sling from the symphysis pubis. However, in our study we measured tape percentile (Hegde et al 2013), i.e., the distance of the midpoint of the sling from the urethrovesical junction divided by the urethral length. We found that when we determined sling location with respect to the urethral length, location had a significant impact on surgical outcomes.
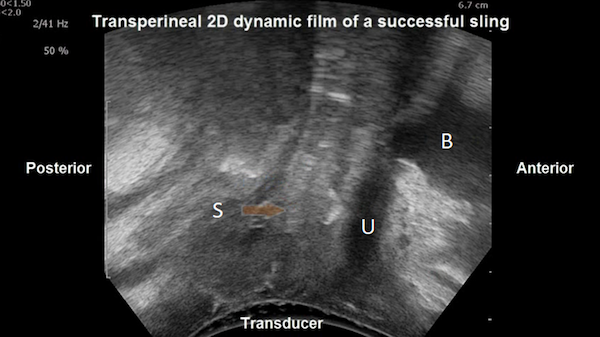
The question that arises is whether there are other ancillary factors that interact with the sling location to ensure continence, especially during dynamic stress like coughing, sneezing, etc. What explains successful outcomes in the small proportion of patients in our study in whom the sling was located proximally and yet reported cure? In an unmatched case-control study of 100 patients returning for their 1–2-year follow-up, we determined, using 2D and 3D transperineal ultrasound studies (Hegde et al 2017), that there are three parameters that interact to ensure success:
1. Deformability of the sling: The dynamic change in shape of the tape in the 2D cineloop film was used to categorize three types of sling deformability:
Figure 4a
Transperineal ultrasound image in the midsagittal plane: transobturator sling is seen to lie midurethrally slightly curved at rest. B: Bladder; U: Urethra; S: Sling
Figure 4b
Transperineal ultrasound image in the midsagittal plane: transobturator sling is seen to lie midurethrally bent into a C shape on Valsalva. B: Bladder; U: Urethra; S: Sling
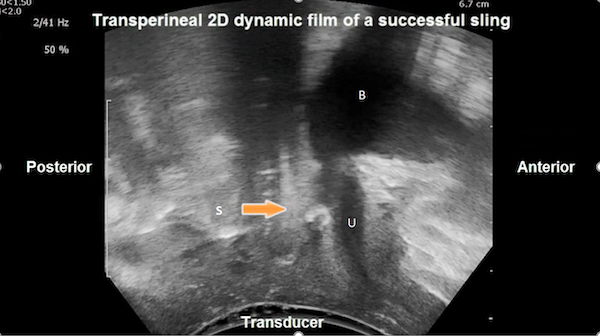
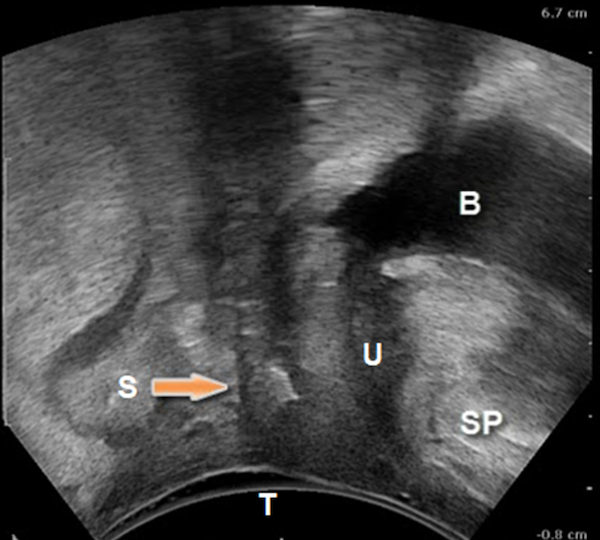
Figure 5
Transperineal ultrasound image in the midsagittal plane: transobturator sling is flat at rest and maximal Valsalva. B: Bladder; U: Urethra; S: Sling; SP: symphysis pubis; T: transducer
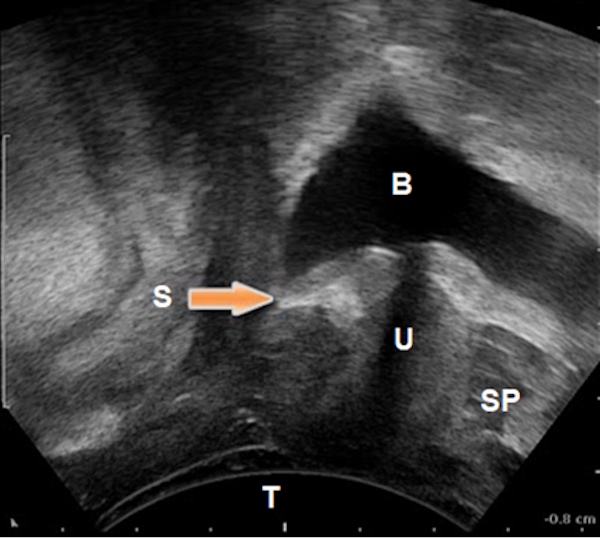
Figure 6
Transperineal ultrasound image in the midsagittal plane: transobturator sling is curved at rest and maximal Valsalva and located proximally. B: Bladder; U: Urethra; S: Sling; SP: symphysis pubis; T: transducer
2. Location of the sling on maximal Valsalva (proximal, mid or distal with respect to the urethral length).
3. Concordance of urethral movement with the sling during maximal Valsalva: If the sling location on maximal Valsalva relative to the urethral length was identical to that at rest, the urethra was considered to move concordant with the sling (Hegde et al 2017; Figures 4a and 4b). If the sling location on maximal Valsalva relative to the urethral length differed from that at rest, the urethral movement in relation to the sling was considered discordant (Hegde et al 2017; Figure 7).
The best outcomes following mid-urethral transobturator sling surgery as well as TVT sling surgery were found to be associated with concordance of urethral movement with the sling and mid-urethral location at maximal Valsalva followed by deformability of the sling on dynamic assessment (Hegde et al 2014). However, the three parameters often work together to compensate for the failure of an individual parameter to ensure successful outcome (Hegde et al 2014). A patient in whom the sling does not deform on Valsalva (i.e., does not curve into a C-shape from flat at rest along its width) may still have a successful outcome if the sling is in the correct location (mid-urethral) at rest and the urethra moves in a concordant manner with the sling (Hegde et al 2014).
When the urethral movement is discordant, i.e., the urethra moves independently of the sling on dynamic assessment, it indicates that the sling has not fixated itself to the suburethral connective tissue. It could also imply that the sling has been inserted too loosely such that even though the sling has scarred in following surgery, there is no tissue bridge between the suburethral tissue and the sling (Hegde et al 2017). Therefore, even if the sling is located mid-urethrally at rest, it cannot cause dynamic compression of the urethra on dynamic assessment as the urethra moves independent of the sling.
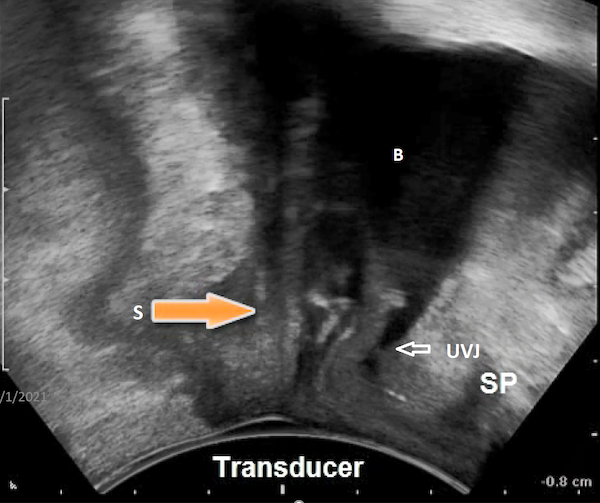
Figure 7
Transperineal ultrasound image in the midsagittal plane on maximal Valsalva: Urethrovesical junction can be seen moving distal to the sling which is fixed in place. Urethra is moving independent of the sling: discordant movement of the urethra with respect to the sling B: Bladder; U: Urethra; S: Sling; SP: symphysis pubis; UVJ: urethrovesical junction
Ascertaining the location of the failed sling may help to elucidate the reasons for sling failure (Hegde et al 2017) and help determine the vaginal incision site if sling takedown is planned. It also helps to understand if sling takedown is required in a case of sling failure: if the proximally located sling is seen to be pulling apart the bladder neck on cough/Valsalva leading to incontinence, sling takedown may be prudent. A distally located sling that is not distorting urethral anatomy may be left in place even if repeat sling surgery is planned.
Determining sling location also helps understand optimal future course of action (Hegde et al 2020). In a patient in whom the previous failed sling is located proximal to the urethrovesical junction, it is akin to starting anew in a treatment-naïve patient because the sling is incorrectly located and thus has no impact on continence in the patient (Hegde et al 2020). However, if continence is slightly improved, if not completely achieved, and the sling is found to be located beneath proximal urethra, there is a possibility that bulking agent injection could be beneficial (Hegde et al 2020). Also, if a repeat sling surgery is planned, determining the location of the previous sling can potentially guide us in identifying the optimal location of insertion of the new sling (Hegde et al 2020).
Dietz HP, Mouritsen L, Ellis G, Wilson PD. How important is TVT location? Acta Obstet Gynecol Scand. 2004;83(10):904–8.
Hegde A, Nogueiras M, Aguilar V, Davila GW. Correlation of static and dynamic location of the transobturator sling with outcomes as described by 3 dimensional endovaginal ultrasound.? Int Urogynecol J. 2013; 24 Suppl. 3: S30.
Hegde A, Nogueiras M, Aguilar V, Davila GW. Dynamic assessment of TVT sling function on transperineal ultrasound: Is it correlated with outcomes one year following surgery? Int Urogynecol J. 2014; 25 Suppl. 4: S34.
Hegde A, Nogueiras M, Aguilar V, Davila GW. Dynamic assessment of sling function on transperineal ultrasound: Is it correlated with outcomes one year following surgery? Int Urogynecol J. 2017; 28:857–864.
Hegde A, Shobeiri SA, Davila GW. Endovaginal Imaging: Slings In: Shobeiri SA, editor. Practical Pelvic Ultrasonography: Springer, New York; 2017. p 209-228.
Hegde A, Davila GW. Does Tape Positioning: Does It Matter? In: Santoro G, Wieczorek AP, Sultan A; eds. Pelvic Floor Disorders. 2020.