Urethral pressure is the fluid pressure required to open a closed urethra (1). The Brown and Wickham technique (2) remains the most recognised method for assessing it. The ICS has published the standardisation of the technique in 2002 (1) but this has not been updated since then. Urethral occlusion can manifest passively e.g. obstructive prolapse, or actively, either involuntarily e.g. bladder neck or voluntarily e.g. sphincter and pelvic floor contraction. Profiles can be measured at rest, under stress (cough test / Valsalva), during pelvic floor contractions or even during the voiding phase.
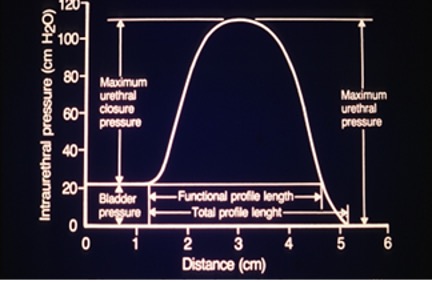
Functional urethral length (FUL), representing the segment where urethral pressure exceeds intravesical pressure, is typically around 3cm and tends to decrease with ageing (3). Maximum urethral closure pressure (MUCP) is the main parameter to be measured. Normal values can be calculated by subtracting the patient's age from 92 (4) or 110 − age ± 20 % (5). In incontinent females, MUCP <20cmH2O is suggestive of intrinsic sphincter deficiency (ISD). Previous anti-incontinence surgery, older age and menopause are risk factors for low MUCP (6). Not only values, but also UPP curve shape can offer clinical insights, i.e. higher pressures at the trace's onset may indicate bladder neck hypertrophy or a dip in the pressure resulting is a double hump could indicate a urethral diverticulum or urethro-vaginal fistula.
Low maximum urethral closure pressure (MUCP) has been significantly associated with stress urinary incontinence (SUI) in several studies (7). According to De Lancey, MUCP was 42% lower in incontinent subjects (8). In a systematic review, MUCP was the strongest determinant of SUI (9) with a specificity of 98% when MUCP <20cmH2O.
Assessment of urethral function is a crucial part of urodynamics and UPPs can play an important role in the prognosis following SUI surgery (10). MUCP has been identified as a potential predictor for post-operative outcomes in several studies and NICE in their 2013 guidelines have highlighted that women with SUI and MUCP <20cmH2O do poorly with supportive procedures such as colposuspension or synthetic tension-free synthetic slings. In a cohort of 565 females, MUCP in the lowest quartile demonstrated a twofold increased risk of objective failure one year after surgery (11). According to Vij et al. surgical success was higher with MUCP of 55cmH2O compared to 35 or lower (12). The retropubic approach has shown a higher success rate in women with poor urethral function compared to the transobturator route (10). Therefore, MUCP can play a role in predicting surgical success and guiding surgical treatment decisions.
In assessing voiding dysfunction, particularly in functional bladder outflow obstruction, UPP can help in patient categorisation. A high MUCP may be present in women with voiding dysfunction, especially Fowler's syndrome where the MUCP is over >100cmH2O (3) and seem to respond better to sacral neuromodulation (13). MUCP has also been considered as the only objective available tool for selecting patients before the off-licence use of sphincter botulinum toxin injection treatment (14). In primary bladder neck obstruction (PBNO), the UPP shape may be modified, as well as pressure values at the bladder neck level. While the role of UPP in dysfunctional voiding is less clear, elevated voluntary pressures, reaching up to 300cmH2O, can be observed in such cases (3).
Despite UPP's diagnostic accuracy, its predictive value and reproducibility are criticised, and it is currently not recommended to grade the severity of incontinence in the European Association of Urology guidelines. The positive attributes of UPP, such as its availability, minimally invasive nature, and cost-effectiveness, should be recognised. The standardisation of technique needs updating and we ought to employ this available tool effectively for a more comprehensive assessment of urethral function and understanding of female LUTS.
ICS UPP Female diagram with recommended nomenclature
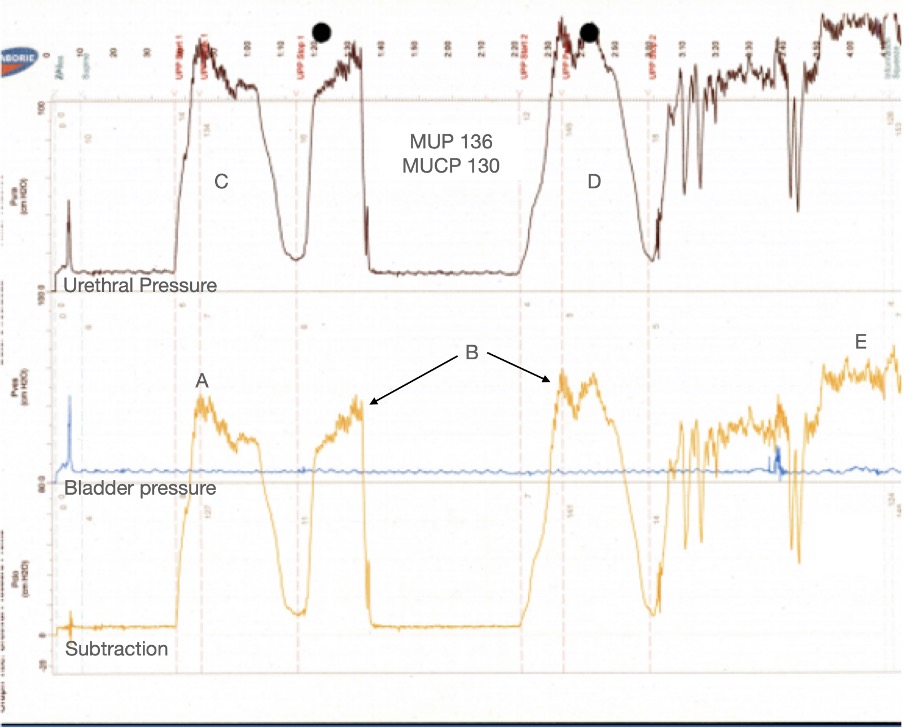
UPP in a 33 y/o female
High MUCP (130 cm H2O) is demonstrated (A)
Vascular pulsations are seen (B)
UPP is done twice (C and D) to compare and have a more reliable information, the average is calculated and reported
(E) Voluntary pelvic floor contraction
References
1. Lose G, Griffiths D, Hosker G, Kulseng‐Hanssen S, Perucchini D, Schäfer W, et al. Standardisation of urethral pressure measurement: Report from the standardisation sub‐committee of the International Continence Society. Neurourol Urodyn. 2002 Jan;21(3):258–60.
2. Brown M, Wickham JEA. THE URETHRAL PRESSURE PROFILE. Br J Urol. 1969 Apr;41(2):211–7.
3. Drake M, Hashim, Hasimm, Gammie Andrew, editors. Abrams Urodynamics. 4th ed. 2021.
4. Edwards L, Malvern J. The Urethral Pressure Profile: Theoretical Considerations and Clinical Application. Br J Urol. 1974 Jun;46(3):325–35.
5. Constantinou CE. Resting and Stress Urethral Pressures as a Clinical Guide to the Mechanism of Continence. Clin Obstet Gynaecol. 1985 Jun;12(2):343–56.
6. Kapoor DS, Housami F, White P, Swithinbank L, Drake M. Maximum urethral closure pressure in women: normative data and evaluation as a diagnostic test. Int Urogynecology J. 2012 Nov;23(11):1613–8.
7. Schick E, Dupont C, Bertrand PE, Jolivet-Tremblay M, Tessier J. Predictive Value of Maximum Urethral Closure Pressure, Urethral Hypermobility and Urethral Incompetence in the Diagnosis of Clinically Significant Female Genuine Stress Incontinence. J Urol. 2004 May;171(5):1871–5.
8. DeLancey JOL, Trowbridge ER, Miller JM, Morgan DM, Guire K, Fenner DE, et al. Stress Urinary Incontinence: Relative Importance of Urethral Support and Urethral Closure Pressure. J Urol. 2008 Jun;179(6):2286–90.
9. Kawasaki A, Wu JM, Amundsen CL, Weidner AC, Judd JP, Balk EM, et al. Do urodynamic parameters predict persistent postoperative stress incontinence after midurethral sling? A systematic review. Int Urogynecology J. 2012 Jul;23(7):813–22.
10. Robinson D, Thiagamoorthy G, Ford A, Araklitis G, Giarenis I, Cardozo L. Does assessing urethral function allow the selection of the optimal therapy for recurrent SUI? Report from the ICI‐RS 2017. Neurourol Urodyn [Internet]. 2018 Jun [cited 2023 Dec 27];37(S4). Available from: https://onlinelibrary.wiley.com/doi/10.1002/nau.23588
11. Nager CW, Sirls L, Litman HJ, Richter H, Nygaard I, Chai T, et al. Baseline Urodynamic Predictors of Treatment Failure 1 Year After Mid Urethral Sling Surgery. J Urol. 2011 Aug;186(2):597–603.
12. Vij M, Dua A, Freeman RM. Should maximal urethral closure pressure be performed before midurethral sling surgery for stress incontinence? A time to revisit. Int Urogynecology J. 2016 Oct;27(10):1491–5.
13. De Ridder D, Ost D, Bruyninckx F. The Presence of Fowler’s Syndrome Predicts Successful Long-Term Outcome of Sacral Nerve Stimulation in Women with Urinary Retention. Eur Urol. 2007 Jan;51(1):229–34.
14. Nadeem M, Lindsay J, Pakzad M, Hamid R, Ockrim J, Greenwell T. Botulinum toxin A injection to the external urethral sphincter for voiding dysfunction in females: A tertiary center experience. Neurourol Urodyn. 2022 Nov;41(8):1793–9.