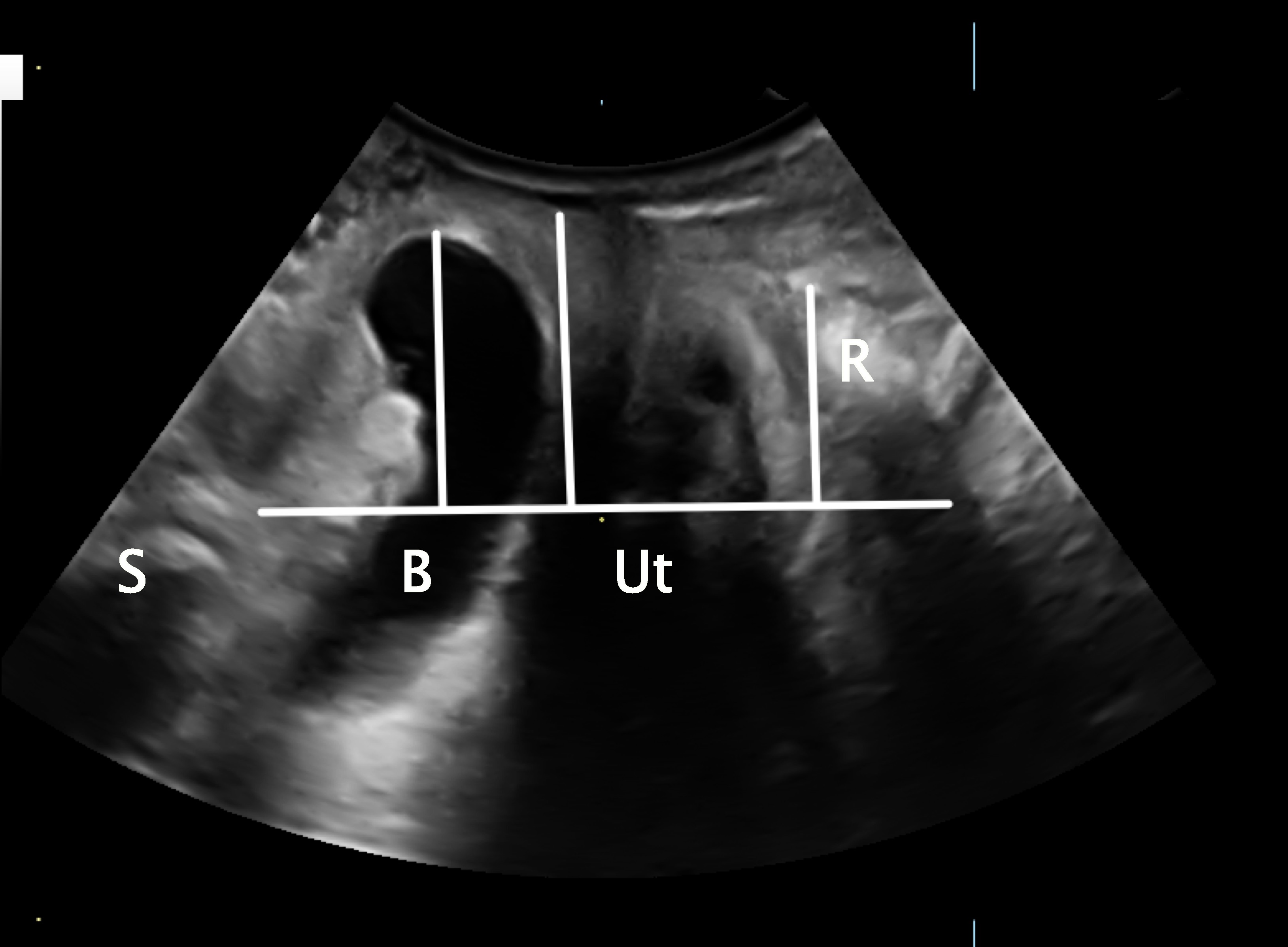
2D/3D endovaginal ultrasonography (EVUS) is the only ultrasound imaging technique that has been validated to visualize structures of the rectovaginal space and the levator ani muscles using histologic and cadaveric correlations (Shobeiri et al 2009; Shobeiri, Rostaminia et al 2012; Shobeiri, White et al 2012). Although perineal ultrasound can be used to evaluate prolapse, it rarely adds to clinical examination. As a matter of fact, prolapse beyond the hymen makes the performance of perineal ultrasound difficult to impossible. Conversely, prolapse reduction by EVUS probe gives a unique advantage to EVUS as the supportive structures are seen clearly. EVUS, by placing a high-resolution 16 MHz probe millimeters away from the structures of interest, can provide views that are comparable to microscopic views of the tissue (Rostaminia et al 2014). EVUS easily evaluates the internal and external anal sphincters (IAS and EAS), levator ani defects (Rostaminia et al 2016; Asif et al 2022), anorectal cysts and fistulas (Shobeiri et al 2013), the rectovaginal septum (RVS), and the levator plate (Jeong et al 2021). It also assesses the functional strength of the pelvic floor (Rostaminia et al 2015) and implanted vaginal mesh (Manonai et al 2015). EVUS has shown that women with obstructive defecatory symptoms (ODS) have a wider rectum and descendent of the levator plate regardless of the prolapse stage as measured by levator plate descent angle and levator plate-probe distance (Rostaminia et al 2019). Female ODS are associated with distinct alterations in rectal mobility and support that can be clearly observed on EVUS. The defects in rectal support were quantifiable using a compression ratio metric. A threshold analysis indicated that the risk of ODS was 32 times greater among women with a high compression ratio (>/= 14) compared with those with a low compression ratio (< 14). EVUS measurements strongly predict the likelihood of symptoms; interestingly, the presence or degree of rectocele defects plays no role (Rostaminia et al 2020). Women with more severe ODS experience more rectal hypermobility/folding as measured by EVUS (Routzong et al 2021).
In summary, EVUS’ image quality surpasses that of perineal imaging and enables measurements of many important rectal parameters. EVUS provides a cheaper, effective alternative to magnetic resonance defecography to evaluate obstructed defecation.
REFERENCES
Asif Z, Tomashev R, Peterkin V, Wei Q, Alshiek J, Yael B, et al. Levator ani muscle volume and architecture in normal vs. muscle damage patients using 3D endovaginal ultrasound: a pilot study. Int Urogynecol J. 2022.
Jeong HY, Park DH, Lee JK. Levator plate descent angle in pelvic floor disorders. Tech Coloproctol. 2021;25(9):1011-8.
Manonai J, Rostaminia G, Denson L, Shobeiri SA. Clinical and ultrasonographic study of patients presenting with transvaginal mesh complications. Neurourol Urodyn. 2015.
Rostaminia G, Abramowitch S, Chang C, Goldberg RP. Descent and hypermobility of the rectum in women with obstructed defecation symptoms. Int Urogynecol J. 2020;31(2):337-49.
Rostaminia G, Javadian P, Awad C, Shobeiri SA. Ultrasound Indicators of Rectal Support Defect in Women With Obstructive Defecatory Symptoms. Female pelvic medicine & reconstructive surgery. 2019;25(3):222-5.
Rostaminia G, Peck J, Quiroz L, Shobeiri SA. Levator Plate Upward Lift on Dynamic Sonography and Levator Muscle Strength. Journal of ultrasound in medicine: official journal of the American Institute of Ultrasound in Medicine. 2015;34(10):1787-92.
Rostaminia G, Peck JD, Van Delft K, Thakar R, Sultan A, Shobeiri SA. New Measures for Predicting Birth-Related Pelvic Floor Trauma. Female Pelvic Medicine & Reconstructive Surgery. 2016;22(5):292-6.
Rostaminia G, White D, Quiroz L, Shobeiri SA. Is a New High-Resolution Probe Better than the Standard Probe for 3D Anal Sphincter and Levator Ani Imaging? Ultrasonic Imaging. 2014.Page? Issue? Vol?
Routzong MR, Abramowitch SD, Chang C, Goldberg RP, Rostaminia G. Obstructed Defecation Symptom Severity and Degree of Rectal Hypermobility and Folding Detected by Dynamic Ultrasound. Ultrasound Q. 2021;37(3):229-36.
Shobeiri SA, Leclaire E, Nihira MA, Quiroz LH, O'Donoghue D. Appearance of the levator ani muscle subdivisions in endovaginal three-dimensional ultrasonography. Obstetrics & Gynecology. 2009;114:66-72.
Shobeiri SA, Rostaminia G, White DE, Quiroz LH. The determinants of minimal levator hiatus and their relationship to the puborectalis muscle and the levator plate. BJOG. 2012;120(2):205-11.
Shobeiri SA, Rostaminia G, White D, Quiroz LH, Nihira MA. Evaluation of vaginal cysts and masses by 3-dimensional endovaginal and endoanal sonography. J Ultrasound Med. 2013;32(8):1499-507.
Shobeiri SA, White D, Quiroz LH, Nihira MA. Anterior and posterior compartment 3D endovaginal ultrasound anatomy based on direct histologic comparison. Int Urogynecol J. 2012;23(8):1047-53.
Posterior compartment abnormalities and bowel symptoms are highly prevalent in the urogynecological population. More than 50% of our patients are diagnosed with significant posterior compartment prolapse, around 60% report obstructive defecation (Guzman Rojas et al 2016) and more than 10% anal incontinence (Guzman Rojas et al 2015). Posterior compartment prolapse can be due to a true rectocele secondary to herniation of the rectal ampulla through a rectovaginal septal defect, an enterocele, a rectoenterocele, rectal intussusception and perineal hypermobility (Figure 2). These conditions may contribute to defecatory disorders and are difficult to differentiate without imaging (Alam et al 2017). Obstetric anal sphincter trauma is one of the main risk factors for anal incontinence (Sultan & Thakar 2002). It is difficult to evaluate anal sphincter anatomy on digital rectal examination without imaging (Shek et al 2016).
Transperineal ultrasound (TLUS) is performed by placing a 2D/3D curvilinear transducer on the perineum. The equipment required for TLUS is easily accessible, the technique is cheap, safe, reproducible (Tan et al 2015; Turel et al 2019) and noninvasive and hence, the technique of choice for pelvic floor imaging. It has been standardized and validated for both pelvic floor (Shek et al 2015; Dietz et al 2010; Dietz et al 2008; Dietz et al 2011; Dietz et al 2007; Dietz et al 2015) and anal sphincter assessment (Guzman Rojas et al 2015; Turel et al 2018; Subramaniam & Dietz 2020). Good agreement has been shown with endoanal ultrasound (Ros et al 2017) and patient acceptance is higher (Taithongchai et al 2019). Unlike endoluminal imaging, TLUS does not cause splinting and does not impede prolapse development and pelvic floor assessment (Hainsworth et al 2015). For anal sphincter imaging, TLUS does not distort anatomy and avoids overestimating the size of sphincter defects. It allows dynamic evaluation of the anal sphincter and mucosa (Dietz 2018). In contrast to endoanal ultrasound, reproducible reference planes are used for anal sphincter assessment, making TLUS less subjective (Figure 3). TLUS can also be used to image the perineum which can be helpful in surgical audits of episiotomy and in understanding patterns of trauma (Figure 4; Subramaniam et al 2021).
Pelvic floor structural changes frequently involve multiple compartments and women usually have a multiplicity of pelvic floor disorders. TLUS allows a comprehensive assessment of the pelvic floor by providing information of the lower urinary tract, the anterior and central compartment as well as the levator ani (Figure 5, Figure 6). While the state of the levator ani seems to have less bearing on colorectal conditions, rectal intussusception is associated with levator avulsion and hiatal ballooning (Guzman Rojas et al 2011) and anal sphincter defects are associated with levator avulsion (Valsky et al 2016). A comprehensive pelvic floor assessment is helpful in understanding pelvic floor functional anatomy and in patient counselling and management.
Apart from diagnosis, TLUS can be used in treatment, e.g., by providing visual biofeedback in obstructive defecation secondary to anismus and in rectal intussusception to advise against straining on defecation.
One may argue that resolution is better with endoluminal imaging of sphincter defects, but it remains to be shown whether this has any impact on the detection of clinically relevant defects. I would like to ask readers to compare the images in this article with those in the recently published document, Consensus Definitions and Interpretation Templates for Dynamic Ultrasound Imaging of Defecatory Pelvic Floor Disorders (Alshiek et al 2023). In my opinion it is plainly obvious that TLUS provides the superior diagnostic option: less investment, better images, and less discomfort for the patient.
REFERENCES
Alam P, Guzman R, Kamisan AI, Mann K, Dietz HP. The ‘bother’ of obstructed defecation. Ultrasound Obstet Gynecol. 2017;49:394-7.
Alshiek J, Murad-Regadas SM, Mellgren A, Glanc P, Khatri G, Quiroz LH, et al. Consensus definitions and interpretation templates for dynamic ultrasound imaging of defecatory pelvic floor disorders. Int Urogynecol J. 2023;34:603-619.
Dietz HP. Exoanal Imaging of the Anal Sphincters. J Ultrasound Med. 2018;37(1):263-80.
20. Subramaniam N, Shek KL, Dietz HP. Imaging Characteristics of Episiotomy Scars on Translabial Ultrasound: An Observational Study. J Ultrasound Med. 2021;41(9):2287-93.
Dietz HP, Bernardo M, Kirby A, Shek KL. Minimal criteria for the diagnosis of avulsion of the puborectalis muscle by tomographic ultrasound. Int Urogynecol J. 2010;22(6):699-704.
Dietz HP, De Leon J, Shek KL. Ballooning of the levator hiatus. Ultrasound Obstet Gynecol. 2008;31:676-80.
Dietz HP, Lekskulchai O. Ultrasound assessment of prolapse: the relationship between prolapse severity and symptoms. Ultrasound Obstet Gynecol. 2007;29:688-91.
Dietz HP, Wong V, Shek KL. A simplified method for determining hiatal biometry. Aust NZ J Obstet Gynaecol. 2011;51(6):540-3.
Dietz HP, Zhang X, Shek KL, Guzman RR. How large does a rectocele have to be to cause symptoms? A 3D/4D ultrasound study. Int Urogynecol J. 2015;26(9):1355-9.
Guzman R, Kamisan AI, Shek KL, Dietz HP. Anal sphincter trauma and anal incontinence in urogynecological patients. Ultrasound Obstet Gynecol. 2015;46:363-6.
Guzman R, Kamisan AI, Shek KL, Dietz HP. The prevalence of abnormal posterior compartment anatomy and its association with obstructed defecation symptoms in urogynecological patients. Int Urogynecol J. 2016;27:939-44.
Guzman R, Shek KL, Dietz HP. Rectal intussusception is associated with abnormal levator structure and morphometry. Tech Coloproctol. 2011;15:39-43.
Hainsworth AJ, Solanki D, Schizas AMP, Williams AB. Total pelvic floor ultrasound for pelvic floor defaecatory dysfunction: a pictorial review. Br J Radiology. 2015;88(1055):20150494. doi:10.1259/bjr.20150494.
Ros C, Martínez-Franco E, Wozniak MM, Cassado J, Santoro G, Elías N, et al. Postpartum two- and three-dimensional ultrasound evaluation of anal sphincter complex in women with obstetric anal sphincter injury. Ultrasound Obstet Gynecol. 2017;49(4):508-14.
Shek KL, Dietz HP. What is abnormal uterine descent on translabial ultrasound? Int Urogynecol J. 2015;26:1783-87.
Shek KL, Kamisan Atan I, Dietz HP. Can Anal Sphincter Defects Be Identified by Palpation? Female Pelvic Med Reconstr Surg. 2016;22(6):472-5.
Sultan AH, Thakar R. Lower genital tract and anal sphincter trauma. [Review]. Best Practice & Research in Clinical Obstetrics & Gynaecology. 2002;16(1):99-115.
Taithongchai A, van Gruting IMA, Volløyhaug I, Arendsen LP, Sultan AH, Thakar R. Comparing the diagnostic accuracy of 3 ultrasound modalities for diagnosing obstetric anal sphincter injuries. 2019;221(2):134.e1-.e9.
Tan L, Shek KL, Kamisan AI, Guzman RR, Dietz HP. The repeatability of sonographic measures of functional pelvic floor anatomy. Int Urogynecol J. 2015;26:1667-72.
Turel F, Shek KL, Dietz HP. How Valid Is Tomographic Ultrasound Imaging in Diagnosing Levator and Anal Sphincter Trauma? J Ultrasound Med. 2018;00:1-6.
Turel F, Subramaniam N, Bienkiewicz J, Friedman T, Dietz HP. How repeatable is assessment of external anal sphincter trauma by exoanal 4D ultrasound? Ultrasound Obstet Gynecol. 2019;53(6):836-0.
Subramaniam N, Dietz HP. Does exclusion of subcutaneous external anal sphincter on exoanal imaging matter? Ultrasound Obstet Gynecol. 2020;55(6):830-34.
Valsky DV, Cohen SM, Lipschuetz M, Hochner-Celnikier D, Daum H, Yagel I, et al. Third- or Fourth-Degree Intrapartum Anal Sphincter Tears Are Associated with Levator Ani Avulsion in Primiparas. J Ultrasound Med. 2016;35(4):709-15.